
Vulvar Cancer: Management Perspective
Written by: Mohammad Daas, Medical Student, Jordan University, Amman – Jordan & Moiad Alazzam Consultant Gynaecological Oncology Surgeon, Oxford-UK
Clinical History & Examination

Mrs. X a 70 years old lady with BMI of 28.16 presented with an exophytic vulvar lesion on the right labia majora, measured 9 cm, bleeding of 3 months, difficulty walking and sitting.
She has history of type 2 diabetes, HTN, hypercholesterolemia and anxiety. She is chronic smoker 5 cigarettes/day, she has no known drug allergies.
Medications: metformin, Ramipril (ACE inhibitor), Fluoxetine, diazepam, simvastatin, paracetamol.
On examination a large right sided labial carcinoma, bleeds upon touch, tender, no extension to the anal sphincter, palpable right inguinal lymph nodes while left side was not palpable (Picture 1)
Investigations
CT scan right abnormal vulva, right lymph nodes, right lower lobe lung nodule, abnormal adrenal gland. However, there was no lung or adrenal mets on PET CT.
Initial diagnostic biopsy confirmed grade 1 vulvar squamous cell carcinoma.
MDT discussion & Plan
Decision to proceed with vulvectomy and groin node dissection with adjuvant radiotherapy consideration after.
Surgical plan and assessment
The patient had Initially “EUA: Examination Under Anaesthesia” jointly carried by the gynae-oncology surgeon & the plastic surgeon.
The outcome of the EUA was that the best surgical approach would be hybrid technique (hemi-butterfly excision) followed by rotational flaps to the vulvar area.
The surgery
The surgical procedure combined two techniques:
- Hemi butterfly to the right side (cancer excision and excision of right groin node en bloc).
- Separate incision to groin nodes on the left side.
The flap & closure technique

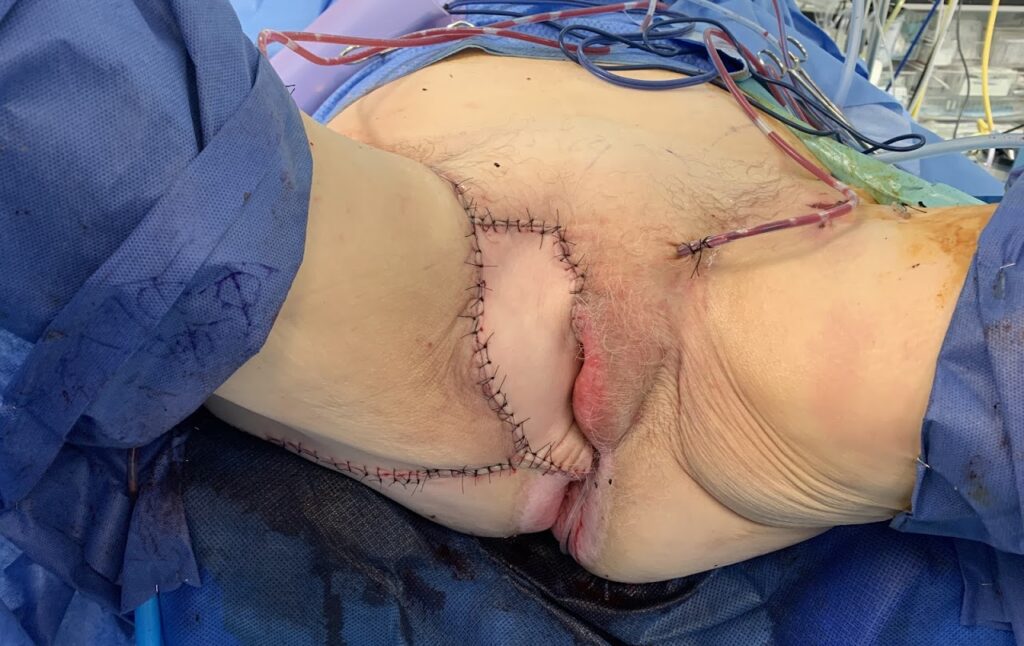
In this patient and as illustrated in the pictures below (Pictures 2 & 3), the final defect was fairly large and not suitable for primary closure. The internal pudendal artery perforator thigh flap (IPAP) was used in order to fill the defect while maintaining the sensation
A major challenge to preserve such flap due to location; pressure prone area, risk of urinary or faecal contamination, and risk of tissue healing due to being a smoker and diabetic. All of the above factors contribute to poor wound healing, breakdown and risk of infection and graft necrosis. In order to avoid the risks of flap failure the following was used:
1. Careful consideration to blood supply and perforators during surgery and flap mobilization. Avoidance of extensive use of diathermy for hemostasis.
2. Use of surgical drains to reduce the risk of heamatoma and lymphedema.
3. Use of topical antibiotic (chloramphenicol).
4. Strict instructions of positioning and avoidance of direct pressure to flap area for 2 weeks (Patient was not allowed to sit on the flap area).
5. Urinary catheter for 6 weeks to reduce irritation and contamination.
6. More importantly, the instructions were clearly communicated to the staff in the ward and to the patient on multiple occasions to ensure clarity and adherence.

Discussion
The mainstay of treatment in vulvar cancer is surgery. In the absence of distant metastasis, stages I-III; surgery is curative. In patients who are medically unfit or with distant metastatic disease surgery can be performed for palliative reasons, but each case should be treated individually.
- For stage 1A cancers wide local excision (WLE) is adequate. In cancers <4cms WLE with sentinel or inguino-femoral lymphadenectomy is the standard therapy. Unilateral or bilateral inguino-femoral node dissection is determined by several factors, most importantly is the proximity of the cancer to the midline.
- For larger cancers > 4 cm radical vulvectomy (hemi-butterfly) full radical vulvectomy is more appropriate to reduce the risk of recurrence.
One of the main factors for successful surgical outcome is careful presurgical treatment, surgeon’s utilization of the anatomical and physiological knowledge to adapt the specific needs of the patient.
The liberal use of flap constructions helps in retaining both aesthetic and functional (such sensation) of the resected area and reduce local scarring.
Wound breakdown and chronic lymphedema remain as a major concern and complication for radical vulvar surgery.
Vulvar Cancer General Information
Epidemiology
- Vulvar malignancy is uncommon.
- 4% of the malignancies of the female genital system.
- 90% of which is squamous cell carcinoma.
- Occurs mainly in postmenopausal women, mean age of 65. However, there is a significant rise in younder women due to HPV related changes.
Incidence
- 1300 new cases yearly in UK, 6100 new cases in the USA.
- UK: 440 deaths yearly, USA: 1300 due to vulvar ca
- 10 years survival rate is 53%
Risk factors:
- Menopausal status & Lichen sclerosis
- Cigarette smoking
- VIN, CIN, immunosuppression, and history of cervical cancer.
- HPV infections specially in young patients; Types 16, 18,31 and 33. (16 and 33 accounts for 55% of HPV induced vulvar malignancy)
Presentation
- Vulvar lump
- Long lasting pruritis
- Bleeding
- Pain.
- Lesions are usually raised, ulcerated, pigmented or warty appearance.
- Most common location is labia majora, mostly unifocal.
Spreading method
- 30% Lymphatic embolization to inguinofemoral lymph nodes.
- 5% to pelvic LN (external iliac group).
- Rarely by direct extension to adjacent structures (vagina, urethra and anus).
- Hematogenous spread to distant sites (Lungs, liver and bones).
Staging
- FIGO or TNM (pathological & surgical staging).
Prognosis: The 5 years survival rate in patients with vulvar cancer
- 80% with no lymph nodes involvement.
- Less than 50% if inguinal nodes are positive.
- 10–15% if iliac or pelvic lymph nodes are positive.
Treatment:
- Surgery: See discussion section above
- Radiotherapy: Can be used either primary treatment or adjuvant after surgery. Main indications for primary radiotherapy:
1- If these surgical approaches risk sphincter damage leading to urinary or faecal incontinence, treatment by radiotherapy should be considered, either with curative intent or to reduce tumour volume to permit less destructive surgery.
2- Individual women who are not fit enough to withstand surgery, even when performed under regional anaesthesia, can be treated with primary radiotherapy.
Follow up:
- The recurrence rate of treated vulvar ca is about 33%
- The follow up plan is to try to detect any recurrence in its early stages.
- The follow up regimen will be each 3 months on the first year and every 6 moths for the next year and then annual checkup.
Anatomy Relations:
- Femoral triangle
- Borders:
- Laterally:Sartorius muscle.
- Medially:Adductor longus.
- Floor:Adductor longus + Pectineus (Medially) and iliopsoas (laterally).
- Superiorly: Inguinal ligament.
- Roof: Skin, superficial fascia, deep fascia.
- Superficial fascia contains (superficial inguinal LN, femoral branch of genitofemoral nerve, branches of ilioinguinal nerve, superficial branches of femoral artery accompanying veins and upper part of great saphenous vein.
- Components:
Medial to lateral : VAN + Lateral cutaneous nerve of the thigh
- V: Femoral Vein
- A: Femoral Artery
- N: Femoral Nerve